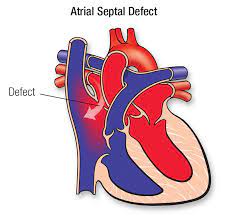
An atrial septal defect (pronounced EY-tree-uhl SEP-tuhl DEE-fekt) is a birth defect of the heart in which there is a hole in the wall (septum) that divides the upper chambers (atria) of the heart.
What is Atrial Septal Defect?

An atrial septal defect is a birth defect of the heart in which there is a hole in the wall (septum) that divides the upper chambers (atria) of the heart. A hole can vary in size and may close on its own or may require surgery. An atrial septal defect is one type of congenital heart defect. Congenital means present at birth.
As a baby’s heart develops during pregnancy, there are normally several openings in the wall dividing the upper chambers of the heart (atria). These usually close during pregnancy or shortly after birth.
If one of these openings does not close, a hole is left, and it is called an atrial septal defect. The hole increases the amount of blood that flows through the lungs and over time, it may cause damage to the blood vessels in the lungs. Damage to the blood vessels in the lungs may cause problems in adulthood, such as high blood pressure in the lungs and heart failure. Other problems may include abnormal heartbeat, and increased risk of stroke.
Causes

Most cases of atrial septal defects occur on their own for no apparent reason (sporadically). The exact nature of the developmental defect or defects that may occur during embryonic development (embryogenesis) remain unclear.
Some cases of ASD appear to run in families. In such rare cases, the two forms, ostium primum and ostium secundum defects seem to be inherited as autosomal dominant genetic traits. To complicate matters further, genetic analysis suggests that there are at least two different genetic disorders involving ASD that are linked to mutations in a gene called
NKX2-5.
Chromosomes, which are present in the nucleus of human cells, carry the genetic information for each individual. Human body cells normally have 46 chromosomes. Pairs of human chromosomes are numbered from 1 through 22 and the sex chromosomes are designated X and Y. Males have one X and one Y chromosome and females have two X chromosomes. Each chromosome has a short arm designated “p” and a long arm designated “q”. Chromosomes are further sub-divided into many bands that are numbered. For example, “chromosome 6p21.3” refers to band 21.3 on the short arm of chromosome 6. Similarly “chromosome 8p23.1-p22” refers to a region between bands 22 and 23.1 on the short arm of chromosome 8. The numbered bands specify the location of the thousands of genes that are present on each chromosome.
Genetic diseases are determined by the combination of genes for a particular trait that are on the chromosomes received from the father and the mother.
Dominant genetic disorders occur when only a single copy of an abnormal gene is necessary for the appearance of the disease. The abnormal gene can be inherited from either parent, or can be the result of a new mutation (gene change) in the affected individual. The risk of passing the abnormal gene from affected parent to offspring is 50% for each pregnancy regardless of the sex of the resulting child.
Recessive genetic disorders occur when an individual inherits the same abnormal gene for the same trait from each parent. If an individual receives one normal gene and one gene for the disease, the person will be a carrier for the disease, but usually will not show symptoms. The risk for two carrier parents to both pass the defective gene and, therefore, have an affected child is 25 percent with each pregnancy. The risk to have a child who is a carrier like the parents is 50 percent with each pregnancy. The chance for a child to receive normal genes from both parents and be genetically normal for that particular trait is 25 percent. The risk is the same for males and females.
All individuals carry 4-5 abnormal genes. Parents who are close relatives (consanguineous) have a higher chance than unrelated parents to both carry the same abnormal gene, which increases the risk to have children with a recessive genetic disorder.
Atrial septal defects may also occur in association with a variety of other congenital heart defects, or in newborns that are relatively small or premature. Ostium primum defects occur frequently in individuals with Down syndrome or Ellis van-Creveld syndrome. (For more information on this disorder, choose “Down” or “Ellis van-Creveld” as your search term in the Rare Disease Database.)
Symptoms

Many babies born with atrial septal defects have no signs or symptoms. Signs or symptoms can begin in adulthood.
Atrial septal defect signs and symptoms can include:
Shortness of breath, especially when exercising
- Fatigue
- Swelling of legs, feet or abdomen
- Heart palpitations or skipped beats
- Stroke
- Heart murmur, a whooshing sound that can be heard through a stethoscope
- When to see a doctor
Contact your doctor if you or your child has:
- Shortness of breath
- Easy tiring, especially after activity
- Swelling of legs, feet or abdomen
- Heart palpitations or skipped beats
Exams and Tests
The health care provider will check how large and severe an ASD is based on the symptoms, physical exam, and the results of heart tests.
The provider may hear abnormal heart sounds when listening to the chest with a stethoscope. A murmur may be heard only in certain body positions. Sometimes, a murmur may not be heard at all. A murmur means that blood is not flowing through the heart smoothly.
The physical exam may also show signs of heart failure in some adults.
An echocardiogram is a test that uses sound waves to create a moving picture of the heart. It is often the first test done. A Doppler study done as part of the echocardiogram allows the health care provider to assess the amount of shunting of blood between the heart chambers.
Other tests that may be done include:
Cardiac catheterization
- Coronary angiography (for patients over 35 years old)
- ECG
- Heart MRI or CT
- Transesophageal echocardiography (TEE)
Treatment
ASD may not need treatment if there are few or no symptoms, or if the defect is small and is not associated with other abnormalities. Surgery to close the defect is recommended if the defect causes a large amount of shunting, the heart is swollen, or symptoms occur.
A procedure has been developed to close the defect (if no other abnormalities are present) without open heart surgery.
The procedure involves placing an ASD closure device into the heart through tubes called catheters.
The health care provider makes a tiny cut in the groin, then inserts the catheters into a blood vessel and up into the heart.
The closure device is then placed across the ASD and the defect is closed.
Sometimes, open-heart surgery may be needed to repair the defect. The type of surgery is more likely needed when other heart defects are present.
Some people with atrial septal defects may be able to have this procedure, depending on the size and location of the defect.
People who have a procedure or surgery to close an ASD should get antibiotics before any dental procedures they have in the period following the procedure. Antibiotics are not needed later on.
Outlook (Prognosis)
In infants, small ASDs (less than 5 mm) will often not cause problems, or will close without treatment. Larger ASDs (8 to 10 mm), often do not close and may need a procedure.
Important factors include the size of the defect, the amount of extra blood flowing through the opening, the size of the right side of the heart, and whether the person has any symptoms.
Some people with ASD may have other congenital heart conditions. These may include a leaky valve or a hole in another area of the heart.
Possible Complications
People with a larger or more complicated ASD are at an increased risk for developing other problems, including:
- Abnormal heart rhythms, particularly atrial fibrillation
- Heart failure
- Heart infection (endocarditis)
- High blood pressure in the arteries of the lungs
- Stroke
- When to Contact a Medical Professional
- Call your provider if you have symptoms of an atrial septal defect.
Prevention
There is no known way to prevent the defect. Some of the complications can be prevented with early detection.
Alternative Names
Congenital heart defect - ASD; Birth defect heart - ASD; Primum ASD; Secundum ASD
Patient Instructions
Pediatric heart surgery - discharge
Comments
Post a Comment